I’ve been silent on the blog for a little bit because I have been putting together a post that doesn’t seems to end. Hopefully I’ll be able to get this all out in one breath – bare with me – here goes …
Week #2 has come and gone in a flash, but not without some interesting cases being read in MRI. I spent the week once again split between Cornell and Columbia Presbyterian Hospital watching my mentor, Dr. Prince, read a variety of cases. For example, we saw cases involving:
- Dilated pancreatic duct
- Kidney and liver transplants (pre- and post-op)
- Multiple cases involving vessel stenoses and aneurisms
- Superficial femoral artery (SFA)
- Multiple bypass grafts
- Pancreatic carcinoma
- Bicuspid aortic valve
- Hepatic and renal cysts
I am quickly learning that a proficient radiologist must have a thorough understanding of human anatomy and physiology as well as insight into the pathology of diseases affecting all organs and tissues. The radiologist’s job can be boiled down to converting pictures to text in the form of reports, which gives the physicians a clear picture of the patient’s status. Even though a picture is worth a thousand words, it is the radiologist’s job to succinctly convey to the physician what is seen in the MRI and provide quantitative measurements of any observations.
Last week I introduced
Contrast-Enhanced MRA and to a lesser extent MRI, which I hope you all are experts in by now. Instead of boring you with more physics and MRI techniques I thought I'd share one of the interesting cases I saw last week:
Transposition of the Great Vessels.
Transposition of the Great Vessels is a condition in which the great vessels (the aorta and pulmonary artery) serving the heart are transposed. In a normal heart, the aorta carries blood from the left ventricle to the body and the pulmonary artery carries blood from the right ventricle to the lungs. In a patient with Great Vessel Transposition, the two main arteries serving the heart are switched forcing blood to circulate in only one of two pathways:
- Oxygenated blood (“Red” blood) is pumped through the left side of the heart to the lungs and back, without entering the rest of the body.
- Deoxygenated blood (“Blue” blood) is pumped through the right side of the heart to the body and back without entering the lungs.
This condition is as serious as it sounds because it destroys the body’s ability to deliver oxygen to the blood serving the entire body. Here is a diagram of the vasculature as it would appear in a patient suffering from Transposition of the Great Vessels:
This is a condition that babies are born with and amazingly, can survive with for a short period of time after birth because of special connections in a newborn heart and blood vessels that help to mix oxygenated and de-oxygenated blood. Generally, babies born with transposition are cyanotic – have blue colored skin, lips, and nail beds – because of low oxygen concentration in the blood.
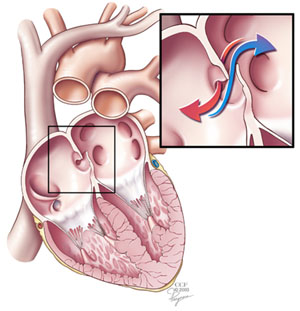
The first connection present in newborn hearts is the foramen ovale or atrial septal defect (ASD), an opening in the atrial septum between the two atria. Here is a diagram of the location of the foramen ovale:
The foramen ovale is used during fetal circulation to speed up the circuit time of blood through the heart. Fetuses don’t use their lungs because they receive oxygen rich blood from the mother via the placenta through the umbilical cord. Blood can therefore be directed straight from the right atria to the left atria without a need to travel through the right ventricle and pulmonary artery.
There is a similar hole in the ventricles referred to as the Ventricular Septal Defect (VSD), which joins the right and left ventricles through a patent hole in the ventricular septum. Just as in the foramen ovale, the VSD helps to mix oxygenated blood into the predominantly deoxygenated blood in the right ventricle and aorta.
Normally, the foramen ovale (and VSD) closes at birth due to increased blood pressure on the left side of the heart. The baby as well as the doctors can take advantage of the foramen ovale to prolong life without the need for major surgery. In some cases where the foramen ovale has already closed, minimally invasive catheterization surgery can be performed to make it patent using a small inflatable balloon similar to balloon angioplasty; The procedure is called a balloon septostomy.
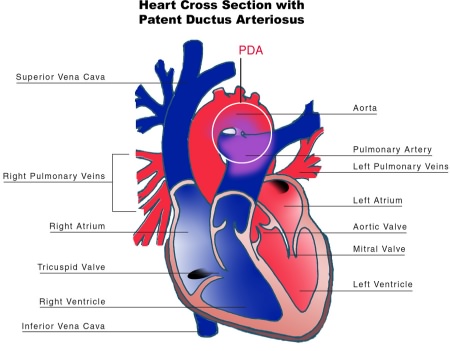
The third life-saving connection in newborns with great vessel transposition is a patent ductus arteriosus, a blood vessel that runs between the aorta and pulmonary artery. Here is a diagram of a patent ductus arteriosus:
As is the case with the foramen ovale, the ductus arteriosus begins to close shortly after the first breath. Generally, the ductus arteriosus completely closes four to ten days following birth. A small connection between the aortic branch and the left pulmonary artery remains after stenosis of the ductus arteriosus and is called the ligamentum arteriosum. Doctors can delay the stenosis of the ductus arteriosus by administering drugs such as Prostaglandin (
Reference).
These three connections aside, no patient can sustain life with transposition of the great vessels because even with patent foramen ovale and ductus arteriosus there isn’t an adequate supply of oxygen to the tissue to maintain its viability, especially considering the added strain of the rapidly developing body.
There are two common surgical procedures used to correct for this malformation of blood vessels:
- Mustard (or Senning) Operation – blood flow is corrected by transposing the pulmonary veins with the systemic veins.
- Fontain Operation – also referred as the Arterial Switch Operation (ASO) – as the name implies this surgical procedure corrects the blood flow by de-transposing the great arteries of the heart.
Choosing the correct surgical procedure can be difficult because there are drawbacks with each. In the Mustard Operation, the procedure is much simpler surgically because veins are much easier to work with. The problem with the Mustard operation is that since the great vessels are still transposed the right side of the heart does the work of the left and vice-versa.
This becomes a problem when considering that each side of the heart performs a different job. The right side is intended to serve the lungs taking in deoxygenated blood from the systemic blood flow and reoxygenating it via the pulmonary arteries. There is considerable less resistance to flow in the right side of the heart and therefore the muscle is weaker than the left.
The left side has a more mechanically stressful job since it is required to push the blood throughout the body. From the start, each side of the heart is designed for different jobs and this means that ultimately the right side of the heart in a patient who has undergone a Mustard operation will fail under the intense stress of the muscle. These patients, whose hearts generally last for 20-30 years, will eventually need a transplant.
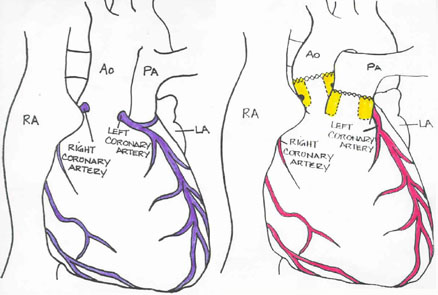
The Fontain or Arterial Switch procedure is more difficult surgically because the surgeon has to separate two major arteries (the aorta and pulmonary artery) from the ventricles and reattach them to the correct ventricle while also moving the coronary arteries, which are significantly smaller (1-2mm in an infant) and very important to proper heart growth and function. The pictures below show the patient’s heart pre- and post-operative. The X denotes the location of surgical stitches.

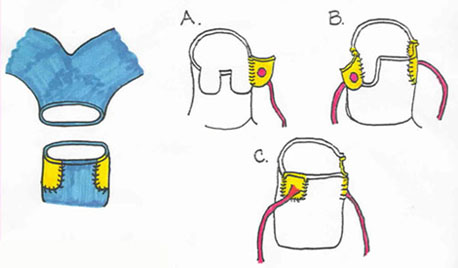
Normally the coronary arteries originate from the ascending aorta immediately distal from the aortic valve. When a surgeon is performing an Arterial Switch Operation (ASO), they must move the coronary arteries from the right side to the left so that the heart muscle receives oxygen-rich blood. To protect the coronary arteries, the surgeon removes a button of tissue surrounding the coronaries to aid in their attachment to the aorta. Here are two diagrams of the changes that are made during surgery:
Essentially, the surgeon excises the aorta and pulmonary arteries just above the valves and frees the coronaries (with additional muscle around it). Next, the surgeon sutures each coronary into place on the left side with fine precision (this can be seen in steps A-C in the first image above). The aorta is then moved into the correct position on the left side of the heart and sutured, above where the coronary arteries were sutured. Next, the two holes in the right side of the heart from the excision of the coronary arteries are patched with pieces of pericardium and the pulmonary artery is attached to the right side (as shown in the left of the first image above). Finally, the foramen ovale and ventricular septal defect are closed and the patent ductus arteriosus is tied off if open.
The surgery is complete but post-operative status is closely watched as complications such as bleeding, and/or myocardial infarction can occur. The patient who I saw this week was scheduled for routine scans to evaluate the condition of his heart. He had undergone a Fontain procedure as a baby and it is common for the patient’s physician to keep a close watch on the health of his heart.
(PAUSE for a quick breath) I guess I couldn’t get it
all out in one breath. I hope that you enjoyed this case, I found it very interesting. Stay tuned for my next novel-length post coming soon!