Medical Databases, Spreadsheets, and Echocardiograms… Oh My!
So with the 4th of July landing on a Tuesday this year, I was given Monday off by my clinician; resulting in a 4 day weekend! This free time allowed me to head off and explore more parts of the city: window shopping on 5th Ave, meandering about the southern part of Central Park, visiting Rockefeller Center, and of course watching more of the World Cup at the ESPN Zone. A group of us got together to watch the fireworks display on the East River from the roof of Olin Hall, which turned out to be quite amazing. After seeing smiley faces and cubes explode in the night sky, Ben decided that if the whole PhD thing does not work out, he’s going into pyrotechnics.
So after a relaxing weekend, I got up bright and early for rounds again with the cardiology residents and fellows in 4 North. The weekend was quite uneventful for the 4 North staff and there were only a few new patients that had been admitted into the ward, but rounds took three and a half hours to get through (in comparison to last week where they only took about two hours). By the end of the rounds, I was feeling more comfortable in understanding all the acronyms that the doctors were using and was beginning to see the standard methodologies used to diagnose and to treat the conditions that the patients had. After rounds I met up with Dr. Weinsaft and was introduced to the patient medical record database that the hospital uses to store all the medical information on all its patients. The database turned out to be very user friendly and accessing the records was easier than I had imagined it would be ( I guess they want to make it as user friendly to the doctors and nurses which have to deal with it on a daily basis, rather than some convoluted CS major’s personal pet project for a CS database class). Through this database I was able to identify over 350 patients that had obtained a cardiac MRI within the last two years. This I then placed into a spreadsheet and was done about two hours later.
Thursday began again with 8am rounds in 4 North, but this time lasting the normal two hours. After rounds, I met up with Dr. Weinsaft once again and we proceeded to read some cardiac MRI images (diagnosing the condition of the patients, determining where the damage had been done during a myocardial infarction (aka a heart attack), and determining the functionality of the viable tissue.) With a few hours spent in a dark room and looking at a computer screen, I moved to another room with another computer screen and began to do more work on compiling the spreadsheet with the patients that we are going to be using for my project. This time I was cross referencing if the patients also had an echocardiogram done in addition to the cardiac MRI. I’ll describe what an echocardiogram is in the following paragraph. After a few hours spent accessing the database, I finished cross-referencing and cut the list down to about 250 patients. Still a lot of patients, but slowly narrowing down the study group that we are going to work with. Later that evening, I was able to finally obtain internet in my dorm room which made life a lot easier by not having to depend on when the library was open. This no longer gives me the excuse to not get work done since I’m jacked into the whole world 24/7.
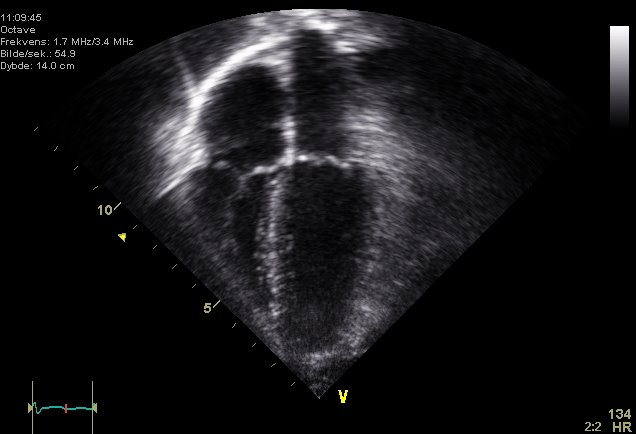
Friday morning began as the last few days have begun, with rounds at 8am in 4 North. Following rounds, I was introduced to the echocardiography staff and sat and watched echocardiograms for the majority of the afternoon. An echocardiogram is another non-invasive method to visualize the heart and to obtain important data that can help diagnose what is happening with the patient. An echocardiogram uses an ultrasound machine (exactly the same type as used to visualize fetuses in pregnant women) to take images of the heart in real-time. Unlike SPECT or CT or cardiac MRI, these images are two dimensional and the visual resolution is not as high, but very important data can still be obtained. The patient comes in and lays down on a table and the technician just takes the ultrasound probe, applies a bit of ultrasound jelly to the chest, and begins to image the heart. The advantage over the other three methods of imaging is that the machine is portable (it does not need a whole room specifically devoted to the instrument), its very quick (the whole procedure is done in about 15 minutes), and to capture the image the patient does not need to hold their breath (to capture a clear image with CT/MRI, you need to hold your breath and lay perfectly still, which is a problem for some patients). An example of an echocardiogram image is shown below, and more information can be found here: http://en.wikipedia.org/wiki/Echocardiography
 http://en.wikipedia.org/wiki/Image:Echocardiogram_4chambers.jpg
http://en.wikipedia.org/wiki/Image:Echocardiogram_4chambers.jpg
After observing eight echocardiograms, I went back to and continued to work on the spreadsheet and continued to narrow down the list of patients that would fit the study. This time I took the 250 patients and read through each medical record to see what type of echocardiogram they had, if the diagnosis had a normal or abnormal heart, and what the EF (ejection fraction: percentage value of blood pumped out from the heart upon systole) value was. From this analysis, I was now able to classify the patients into two groups: those with normal heart and those with abnormal ones. This refined spreadsheet will be analyzed again on Monday and a few more criteria will be added to narrow down the number of patients. From this final spreadsheet, we will choose a number of patients to perform our study on.
This weekend was another adventure in the city with excursions into the central part of Central Park, exploring the West Side of Manhattan, heading to the West side to party at a few clubs, and culminating back at the ESPN Zone in Times Square to watch the Finals of the World Cup. The whole building was packed with French and Italian fans with Italy finally winning with penalty shots. And with that, rounds begin anew tomorrow at 8am.
So after a relaxing weekend, I got up bright and early for rounds again with the cardiology residents and fellows in 4 North. The weekend was quite uneventful for the 4 North staff and there were only a few new patients that had been admitted into the ward, but rounds took three and a half hours to get through (in comparison to last week where they only took about two hours). By the end of the rounds, I was feeling more comfortable in understanding all the acronyms that the doctors were using and was beginning to see the standard methodologies used to diagnose and to treat the conditions that the patients had. After rounds I met up with Dr. Weinsaft and was introduced to the patient medical record database that the hospital uses to store all the medical information on all its patients. The database turned out to be very user friendly and accessing the records was easier than I had imagined it would be ( I guess they want to make it as user friendly to the doctors and nurses which have to deal with it on a daily basis, rather than some convoluted CS major’s personal pet project for a CS database class). Through this database I was able to identify over 350 patients that had obtained a cardiac MRI within the last two years. This I then placed into a spreadsheet and was done about two hours later.
Thursday began again with 8am rounds in 4 North, but this time lasting the normal two hours. After rounds, I met up with Dr. Weinsaft once again and we proceeded to read some cardiac MRI images (diagnosing the condition of the patients, determining where the damage had been done during a myocardial infarction (aka a heart attack), and determining the functionality of the viable tissue.) With a few hours spent in a dark room and looking at a computer screen, I moved to another room with another computer screen and began to do more work on compiling the spreadsheet with the patients that we are going to be using for my project. This time I was cross referencing if the patients also had an echocardiogram done in addition to the cardiac MRI. I’ll describe what an echocardiogram is in the following paragraph. After a few hours spent accessing the database, I finished cross-referencing and cut the list down to about 250 patients. Still a lot of patients, but slowly narrowing down the study group that we are going to work with. Later that evening, I was able to finally obtain internet in my dorm room which made life a lot easier by not having to depend on when the library was open. This no longer gives me the excuse to not get work done since I’m jacked into the whole world 24/7.
Friday morning began as the last few days have begun, with rounds at 8am in 4 North. Following rounds, I was introduced to the echocardiography staff and sat and watched echocardiograms for the majority of the afternoon. An echocardiogram is another non-invasive method to visualize the heart and to obtain important data that can help diagnose what is happening with the patient. An echocardiogram uses an ultrasound machine (exactly the same type as used to visualize fetuses in pregnant women) to take images of the heart in real-time. Unlike SPECT or CT or cardiac MRI, these images are two dimensional and the visual resolution is not as high, but very important data can still be obtained. The patient comes in and lays down on a table and the technician just takes the ultrasound probe, applies a bit of ultrasound jelly to the chest, and begins to image the heart. The advantage over the other three methods of imaging is that the machine is portable (it does not need a whole room specifically devoted to the instrument), its very quick (the whole procedure is done in about 15 minutes), and to capture the image the patient does not need to hold their breath (to capture a clear image with CT/MRI, you need to hold your breath and lay perfectly still, which is a problem for some patients). An example of an echocardiogram image is shown below, and more information can be found here: http://en.wikipedia.org/wiki/Echocardiography
 http://en.wikipedia.org/wiki/Image:Echocardiogram_4chambers.jpg
http://en.wikipedia.org/wiki/Image:Echocardiogram_4chambers.jpgAfter observing eight echocardiograms, I went back to and continued to work on the spreadsheet and continued to narrow down the list of patients that would fit the study. This time I took the 250 patients and read through each medical record to see what type of echocardiogram they had, if the diagnosis had a normal or abnormal heart, and what the EF (ejection fraction: percentage value of blood pumped out from the heart upon systole) value was. From this analysis, I was now able to classify the patients into two groups: those with normal heart and those with abnormal ones. This refined spreadsheet will be analyzed again on Monday and a few more criteria will be added to narrow down the number of patients. From this final spreadsheet, we will choose a number of patients to perform our study on.
This weekend was another adventure in the city with excursions into the central part of Central Park, exploring the West Side of Manhattan, heading to the West side to party at a few clubs, and culminating back at the ESPN Zone in Times Square to watch the Finals of the World Cup. The whole building was packed with French and Italian fans with Italy finally winning with penalty shots. And with that, rounds begin anew tomorrow at 8am.
posted by Jan Kostecki at 11:54 AM
1 comments
![]()
![]()